Low back pain is very common. The vast majority of people reading this sentence have had low back pain at some time in their lives. It is one of the most common reasons for physician visits in the U.S. and results in an estimated $100 billion in annual costs. Given the very high prevalence of low back pain, you would think that we would already have noninvasive treatments that are proven to be safe and effective. You’d be wrong.
Recently the American College of Physicians (ACP) reviewed existing studies about noninvasive treatments for low back pain. (Noninvasive means that they did not consider surgery or injections. These invasive treatments are required in only a small minority of cases.) In February the APC used this evidence review to publish new recommendations for the treatment of low back pain.
For patients with acute (less than four weeks) or subacute (four to twelve weeks) low back pain, the ACP recommendations remind us that most patients improve regardless of treatment. Treatment without medication is recommended first (for example, with superficial heat). If medications are desired by the patient and the physician, nonsteroidal anti-inflammatory drugs (NSAIDs) and muscle relaxants are recommended.
For patients with chronic (longer than twelve weeks) low back pain, the ACP again recommends nonpharmacological treatment with exercise, rehabilitation programs, acupuncture, or mindfulness-based stress reduction. If that doesn’t help, the first-line medicines to consider are NSAIDs. The second line medications are tramadol (Ultram) or duloxetine (Cymbalta). Opioids should only be considered in patients for whom the above options have been ineffective and if the potential benefits outweigh the risks for the individual patient.
The recommendations above are based on moderate-quality evidence. (The ACP uses a formal ranking of the quality of evidence in the studies reviewed.) Some of the recommendations are based on low-quality evidence, which I didn’t include above.
The striking difference between the current recommendations and the previous ones is that medications are no longer recommended as first-line treatment. This isn’t because the nonpharmacological treatments are proven to be so effective. It’s because we’ve learned how modestly effective medication is for low back pain, and we’ve come to appreciate the side effects that medications can cause.
So these are not so much new recommendations about new effective treatments for low back pain, but rather a retraction of the prior recommendations because of how much we realize we don’t know. The recommendations don’t include any high-quality evidence, because there have been no large well-designed randomized trials evaluating various therapies for low back pain.
The bottom lines are these. For chronic low back pain none of the known therapies are extremely effective, and all medications have side effects, so the prevailing philosophy is: if you’re going to prescribe placebo, at least make it a safe one. For acute and subacute back pain, almost everyone gets better regardless of treatment. So the best treatment is time. Perhaps that’s why we call you patients.
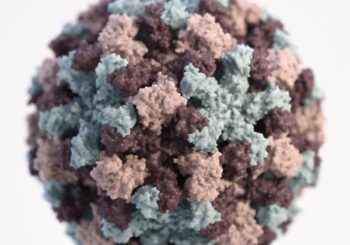
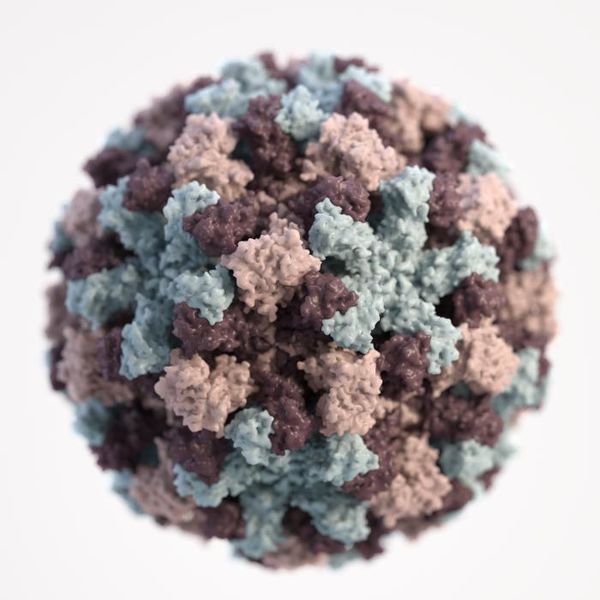
A 3D graphical representation of a single norovirus particle. The different colors represent different regions of the organism’s outer protein shell. Credit: CDC
My longtime readers know that I love to inform you about ways that Mother Nature tries to hurt us. Since it’s winter, norovirus deserves our attention as it wreaks its seasonal havoc and occasionally closes down schools.
Norovirus causes inflammation of the stomach and intestines. It’s commonly referred to as a “stomach virus” or “stomach flu”. (But it’s not related to the influenza virus. So let’s stop calling it the stomach flu. It just confuses people and makes them think that the flu vaccine should have protected them from norovirus, or that anti-flu medication might be effective for it.)
Norovirus illness is not subtle. It causes nausea, vomiting, watery diarrhea and abdominal cramps. Some people also have low-grade fever, headache, and body aches. Symptoms last 24 to 72 hours and most people recover without any lasting harm. But those 24 to 72 hours can cause serious dehydration, and young children, old people, and people with immune defects can get very sick and require hospitalization.
Norovirus makes about 20 million people sick every year in the US, causes over 1 million doctor visits, about 60,000 hospitalizations, and over 500 deaths. You’ve probably already had it, and the majority of us will contract it multiple times. There’s no specific treatment for it. Rehydration is essential, and patients who can’t take oral fluids may need intravenous fluids and intravenous anti-nausea medication.
There are two features of norovirus that makes it an especially prevalent pathogen. The first is that there are very many strains. So you can get sick from norovirus more than once.
The second is that it’s extremely contagious. It makes tuberculosis and viral hepatitis look like they’re playing hard to get. Infected people shed virus in their vomit and their stool and continue to be infectious for a couple of days after they recover. The virus survives on surfaces for weeks and can be ingested in contaminated food or water. Ingestion of a tiny number of virus particles is all it takes to get infected, thereby turning another host into a very sick virus fountain.
This is the virus that spreads like wildfire through cruise ships and schools and other settings in which people eat in close quarters. This winter several school systems have closed for a few days because of the high number of sick students.
What can you do to avoid norovirus this winter? Wash your hands frequently with soap and warm water for at least 20 seconds, especially before eating or preparing food and after using the bathroom. (Hand sanitizers are great for killing bacteria but don’t kill norovirus.) Don’t touch your mouth. If someone is sick at home, have them use their own bathroom if at all possible. Launder and machine-dry any of their soiled clothes and linens. Wipe down surfaces with a bleach-based cleaner. Rinse fresh fruits and vegetables before eating them.
This video from the Centers for Disease Control (CDC) has a great summary of how norovirus is transmitted and how to avoid it. (Of all the videos I’ve seen that were made by an official government agency, I think this is the one that most uses the word “poop”.)
So please stay healthy. And the next time your friend waxes eloquently about nature’s splendor and benevolence, remind him of norovirus.
Ibuprofen tablets Photo credit: Wikimedia / public domain
Non-steroidal anti-inflammatory medicines (NSAIDs) have been around since the 1960s. They include ibuprofen (Advil, Motrin), naproxen (Aleve), meloxicam (Mobic), diclofenac (Voltaren) and over a dozen others. NSAIDs are used to treat pain, decrease fever, and decrease inflammation. They are prescribed over 100 million times annually in the US. Naproxen and ibuprofen are also available over the counter.
NSAIDs were a boon compared to the medications that were available before them. They are more effective for pain than acetaminophen (Tylenol), and are not addictive like opiates. But they do have some side effects. They decrease platelet function and thereby increase bleeding risk, and they can irritate the stomach lining and even cause ulcers. They can also cause kidney injury. These risks are quite small when used for the occasional headache or muscle sprain, but some patients require long-term daily pain medication. These patients’ risk of stomach bleeding from NSAIDs is substantial.
To address this risk, a novel family of medications emerged in the 1990s – COX-2 inhibitors. These medications were designed to have the analgesic and anti-inflammatory benefits of NSAIDs with much lower gastrointestinal risks. In the US two COX-2 inhibitors became available, celecoxib (Celebrex) in 1998 and rofecoxib (Vioxx) in 1999. But Vioxx was found to increase the risk of stroke and heart attack in patients taking it daily and was withdrawn from the market in 1999.
Thereafter it was discovered that traditional NSAIDs likely also increased stroke and heart attack risk somewhat, but the assumption was that Celebrex increased stroke and heart-attack risk more than NSAIDs because it was in the same family as Vioxx. After Vioxx’s withdrawal, the FDA allowed Celebrex to continue to be sold as long as its effect on stroke and heart attack risk was systematically evaluated. The resulting ten-year study was published in November in the New England Journal of Medicine (NEJM).
The study randomized over 24,000 patients who required daily pain medication for arthritis. (Patients for whom Tylenol was sufficient were excluded.) The patients all had some risk factors for heart disease or stroke. They were randomized to receive celecoxib (Celebrex), ibuprofen, or naproxen. Notably, they were all given esomeprazole (Nexium), a strong acid-blocker, to decrease the risk of developing ulcers. They were treated with these medications for about two years on average and were followed for a few years thereafter. The incidence of stroke, heart attacks, intestinal bleeding, kidney injury and other adverse events were tracked. The patients were also asked about the severity of their arthritis pain.
The results were surprising. The patients receiving Celebrex had strokes and heart attacks at similar rates as the patients receiving ibuprofen or naproxen. There was no evidence of higher stroke or heart attack risk with Celebrex. As expected, the patients taking Celebrex had fewer gastrointestinal side effects than those taking the other medicines. Celebrex was also safer than ibuprofen in terms of kidney injury, but similar to naproxen. The patients achieved very similar levels of pain relief, with the patients receiving naproxen having slightly better relief than those receiving Celebrex or ibuprofen.
Some cardiologists criticized the results, arguing that although the trial was supposed to study patients at high risk for stroke and heart attack, the number of actual heart attacks and strokes observed were quite low, suggesting the study enrolled patients at much lower risk than intended. Still, in the population studied, Celebrex resulted in no more strokes or heart attacks than naproxen or ibuprofen.
The generalizable message is that all pain medications have side effects. For the occasional ache and pain, almost any choice is safe. If prolonged daily pain medication is required, try acetaminophen (Tylenol) first. (Tylenol has important liver and kidney risks that you should discuss with your doctor if you’ll be taking it daily.) If acetaminophen is ineffective, Celebrex (celecoxib) or an NSAID is a reasonable next choice. Celebrex is much less likely to lead to gastrointestinal bleeding. If you take Celebrex or an NSAID daily for weeks or longer, a daily antacid in the proton pump inhibitor (PPI) family is important to protect your stomach. Whichever medication you take, try to find the minimum effective dose and take it for the shortest possible duration.
US Surgeon General Vivek Murthy Photo credit: Wikimedia Commons, public domain
In 1964 the Surgeon General issued a report on smoking, summarizing the scientific evidence demonstrating the health risks of tobacco use. Scientifically, nothing in that report was new. It was a review of what was already known. But it had a profound societal effect by publicizing a health risk that had been until then largely ignored. Education, health policy, and the advice of many individual doctors were transformed.
This week the Surgeon General released a report about drug and alcohol misuse and addiction. Like the 1964 report, there is nothing scientifically new. But it is a sobering reminder of the scale of the addiction epidemic that we face.
The annual deaths from alcohol misuse has climbed to 88,000 in the US, and the number of deaths from drug overdoses to 47,000. Both are higher than the number of deaths from car accidents. Almost 21 million people in the US have a substance use disorder, which is about the same as the number with diabetes, and more than the number with all types of cancer combined. Alcohol and drug misuse cost the US more than $400 billion annually in health care, criminal justice, and lost productivity. Prescription pain medications are a big part of the problem. There were 259 million prescriptions written in 2015 for opiate pain medications. There were almost 30,000 lethal overdoses in 2014 due to heroin and pain medicines.
Public understanding and political reaction to this epidemic have been slow to build, partially because of the mistaken perception that it affected primarily the poor. (Even if true, this would be a terrible reason to disregard the problem.) But as the report shows, substance misuse affects all socioeconomic and ethnic groups. It affects our cities and our rural areas. It affects our slums and our elite exurbs.
But the report also highlights some reasons for optimism. Research has brought us more knowledge than ever about the biology, psychology and sociology underpinning the prevention, treatment, and recovery of substance misuse. Addiction is a chronic but treatable psychiatric disease that responds to behavioral and medical intervention. Effective community-based programs exist, but in woefully inadequate supply, and only about 1 in 10 people with a substance use disorder receives any type of treatment. Part of the problem of course, is that many who need treatment believe that they don’t.
The pathway forward is likely to be exceedingly complex. Making significant progress will likely require treatments that address medical, behavioral, and social problems. Acute treatment of addiction is well understood and simply needs to be delivered to many more people. The challenge of prevention is convincing kids who know only addicts that there is another path. The challenge of recovery is constructing support systems that can persuade recovering addicts to postpone their relapse for one more day.
If we are diligent and fortunate, perhaps in 50 years we will look back on this report as the turning point in this national epidemic.
“To die: to sleep;
No more; and by a sleep to say we end
The heart-ache and the thousand natural shocks
That flesh is heir to, ’tis a consummation
Devoutly to be wish’d.”
— Hamlet, Shakespeare
The California End of Life Options Act became effective in June. Before we can understand what the new law permits and how it might change the care of dying patients, we have to understand a little about end of life care prior to this development.
Suffering and dying is not a recent problem. Much has been thought and written about the alleviation of suffering and the medical care of dying patients. This is a well established topic in medical ethics that has been largely reflected in the relevant laws in many states.
So let’s imagine that we are quite ill, and that the pain and debility caused by our illness make us believe that death is preferable to our current state. Prior to the new law, what options were available to us?
One option is refusal of some medical care. This option is based on the general ethical principle of autonomy, which states that an informed patient who is able to make decisions may refuse any care, including life-saving care. So in our example, we may refuse life-saving antibiotics in the event of an overwhelming infection. We may choose not to be hospitalized the next time we are critically ill. We may decide ahead of time that if our breathing or heart were to stop, we would forego artificial respiration or CPR. This general approach allows patients to declare that they are unwilling to undergo some interventions even if these are necessary to prolong their lives.
In practical terms this is done through a conversation between a patient and her physician. These decisions can be formalized in various ways for communication with other doctors and other facilities. A standard way to document these decisions is the Physician Orders for Life-Sustaining Treatment (POLST) form. If you want to document your wishes about life-sustaining treatment, ask your doctor to sit down with you and complete a POLST form.
A second option in our hypothetical example is comfort or palliative care. In some circumstances this is also called hospice care. In comfort care, the emphasis of care is shifted to alleviating distressing symptoms, such as pain and shortness of breath. The ethical principle of beneficence states that physicians are mandated to attempt to alleviate their patients’ suffering. In fact, if the patient’s goal is alleviation of suffering and not prolongation of life, the physician may give medication that relieves the patient’s symptoms even if that medication hastens death. This is permissible because of the principle of double action. The principle of double action states that if an action (the giving of a medication) has two consequences, one of which is desirable (alleviation of pain) and the other one is not (the hastening of death), it may be permissible to take the action. The hastening of death is not taken to be the desired effect of the medication, but an unavoidable consequence of the necessity to treat the pain. Hospice care is therefore not considered assisted suicide or euthanasia, because the primary intent is always the reduction of suffering, not the ending of life. (Euthanasia therefore involves giving lethal drugs with the primary intention of ending life, regardless of whether the patient is currently suffering.)
So in our hypothetical example we could tell our doctor that we choose comfort care. Attempts to diagnose and treat our problems would then stop, and all focus would shift towards keeping us comfortable.
And that was the state of end of life care since I trained about twenty years ago until this June. Assisted suicide was illegal, as was suicide.
Bear with me for a brief digression about suicide. The reason suicide is illegal isn’t to punish suicidal people. The reason suicide is illegal is that the vast majority of people who attempt suicide have a treatable mental illness. After treatment they are usually happy that they were stopped from killing themselves. Suicide is against the law simply to provide a legal framework to stop mentally ill people from doing something irreversible that we suspect they won’t want to do once they are healthy.
I’m certainly not an expert in end of life care, but I do a lot of it. One of the first things primary care doctors learn is that all of our patients will die. So I’ve taken care of a lot of dying patients. The process doesn’t always work perfectly, and any human system will involve mistakes, but I have yet to see a patient whom I believed could not be kept comfortable through excellent hospice care. In my experience, patients who want to die are either depressed or have pain (or some other distressing symptoms like shortness of breath). These are treatable conditions. And we should remember that pain and shortness of breath can be treated with unlimited aggressiveness until either comfort or death is achieved.
Depression, of course, is a more difficult problem, but there are many treatments available for that as well, even for patients in whom medications are not effective. And in any case, patients with severe depression are generally not considered to be capable of making decisions about their death.
So to imagine a patient who might rationally require assisted suicide we have to imagine someone whose symptoms are well controlled (because if not, we can just give them more medication) yet still finds his current state intolerable and less preferable than death. I’ve never seen such a patient, but again, I’m not an expert. I can certainly state that such conditions are extremely rare.
In my training in medical ethics during medical school and residency, I was taught that assisted suicide was not ethical. First, there are myriad ways that it could be abused to prey on the poor (to minimize costs) and the powerless (to minimize hassles). Second, intentionally ending life is outside the goals of medicine. We’re supposed to cure or treat disease, restore function, and alleviate suffering. We’re not supposed to intentionally kill people. Whether or not the patient wants to die is irrelevant. Patients frequently demand things from us (habit forming medications, unindicated surgeries) that are against their interests, and we have an ethical duty to refuse.
So ever since I trained I have believed that assisted suicide was both unethical and also virtually never necessary.
Thanks for bearing with me so far. Let’s turn now to the California End of Life Options Act and understand what it allows.
The new law allows for specific circumstances under which a patient may request, receive, and ingest a drug intended to end his life. (The language in the law is rather Orwellian. The drug used to intentionally end the patient’s life is called an “aid-in-dying drug”. Did the word “poison” sound too unhealthy?) Patients who pursue this option must be residents of California who are 18 years or older, have a terminal incurable disease expected to result in death within six months, be able to make and communicate medical decisions, and be physically capable of swallowing the drug. (The specific identity of the drug is not mandated by the law.)
The patient must make three requests for the lethal drug to his attending physician. Two requests must be made orally at least 15 days apart. The other request must be made in writing on a specific form that is witnessed. The patient must then see a second physician who confirms the terminal diagnosis and that the patient is qualified to receive the lethal drug. The attending physician may then prescribe the lethal medication, after discussing with the patient how to store and administer the drug. Prior to receiving the prescription, the patient is given an opportunity to rescind his request and is encouraged to enroll in hospice. The patient agrees to ingest the drug in a private place with another person present. Participation in this option is completely voluntary for patients and physicians.
For the reasons I’ve already detailed, I believe that patients who will be able to take this new option will be extremely rare. Patients with only several months to live who have decision-making capacity (and maintain that capacity over 15 days) are rare enough. Add to that the requirement that the medication be self-administered, and the law is selecting for an extremely healthy dying person. I can imagine a rare patient with ALS or with a catastrophic malignancy meeting these criteria, but I suspect most of them will still opt for hospice care. And once their disease is advanced enough, they won’t be able to communicate their decision or swallow pills.
Time will tell how many patients pursue this option, and in what circumstances. Time will tell whether the many reasonable safeguards against abuse will operate as intended, or whether doctors cut corners and fudge the facts. Time will tell whether ethicists find legitimate medical principles to support this practice, or continue to argue against it, or shrug and yield to the new legal norm.
I’m willing to keep an open mind and learn from what happens next. I’ll be especially interested to read the arguments of doctors, ethicists, and religious leaders on this issue. But for the time being I believe that this is wrong. I’ll treat patients who ask about it with compassion and professionalism. I’ll point them to the information they want and to doctors who can help them. But when it comes to intentionally killing patients, you can count me out.
“But when you talk about destruction
Don’t you know that you can count me out”
— Revolution, The Beatles
Every year I write a post in the late summer letting you know that flu season is approaching and to get a flu shot. I try to keep my posts informative and evidence-based, but I don’t have anything new to tell you about that.
Actually, I do have one bit of news. Some of you may have heard of FluMist, the flu vaccine given by nasal spray. It’s especially popular with children and with patients with needle phobias because it’s not injected. The Centers for Disease Control and Prevention (CDC) tracks the effectiveness of flu vaccines every flu season. In the 2015-2016 season FluMist offered essentially no protection against the flu, and this followed the previous two seasons in which its effectiveness was much lower than expected. So the CDC is recommending against using FluMist during the 2016-2017 flu season. That’s bad news for patients who might have difficulty receiving injections.
If you want to know which groups of people should have the flu shot and which groups should avoid the flu shot, see my post in 2012. If you’re over 6 months old, you should probably have one. If you want to read my responses to frequently raised objections to the flu shot, see my post from last year.
So, since I’m out of evidence-based information about the flu shot, I present my uninformative and evidence-free top ten reasons to get your flu shot.
10. How else will you be able to spend more time with a friendly medical assistant?
9. The CDC wants you to.
8. Your mother wants you to.
7. If you get sick, you’ll infect Uncle Irving at Thanksgiving, upsetting your mother.
6. Having a needle stuck in your deltoid is fun!
5. If you take more sick days, your boss will forget who you are.
4. It’s easier than wearing a HazMat suit every time you ride the bus.
3. Dave Barry’s article about the Martian Death Flu terrified you.
2. If you don’t, the week of high fever, body aches, and cough will pale next to the months of regret.
And the number one reason to get a flu shot: It will briefly distract you from the election.
Our shipment of flu shots came in this week. Please make an appointment to get yours.
Which animal has killed more people than any other?
Sharks? Sharks are terrifying, right? Nah. They’re not even in the top ten people-killers. They kill about 10 people per year worldwide. Lions? They do a little better with about 100 deaths per year. Snakes are in third place, killing about 50,000 annually.
The number one animal killer of humans is the lowly mosquito which racks up a staggering 750,000 human deaths every year. Mosquitoes achieve the vast majority of those deaths by transmitting malaria, but they also transmit dengue fever, yellow fever, West Nile virus, chikungunya and lots of other diseases that make us sick and sometimes make us dead.
(In second place are humans, who kill about 475,000 other humans annually. It would be nice if one day we could figure out how to kill fewer people than snakes do, thereby sinking to third place.)
In January I wrote about Zika virus, a virus spread by mosquitoes, which at the time was spreading through Latin America and the Caribbean. Zika most commonly causes fever, rash, joint pain and conjunctivitis (pink eye). The illness is usually mild, and many infected people may have no symptoms at all. But in infected pregnant women Zika virus can cause miscarriages and serious birth defects. And very rarely Zika can cause Guillain-Barré syndrome, a disorder that results in temporary paralysis.
This year Zika virus has spread further across Latin America and the Caribbean, including Puerto Rico. As of July 27 there were about 1,600 cases of Zika in the U.S., virtually all of them acquired during travel to infected areas, none acquired here.
That changed last week when the Centers for Disease Control (CDC) reported that 4 cases of Zika were identified in Miami which were unrelated to travel. Since then a total of 15 cases have been identified in a Wynwood, a neighborhood in Miami. These cases appear to have been acquired through local transmission, that is, mosquitoes spreading the virus from person to person.
Health officials are aggressively implementing measures to decrease the mosquito population in Wynwood, like eliminating standing water and spraying insecticide. But so far their effect on the mosquito population has been only modest.
It is entirely possible that Zika may spread from Miami to other warm and humid U.S. cities that are hospitable to mosquitoes. Though the illness is almost always without lasting consequences, the possibility of birth defects would pose a serious risk if Zika became more widespread in the U.S. Work has commenced on a vaccine, but that is at least a year away.
But there is a tested technology that may be just the thing to beat Zika back. The British biotech firm Oxitec has developed a genetically modified (GM) mosquito that they would like to release as a test in the Florida Keys. The modified mosquito has only two differences from the mosquito in the wild. The first is a gene that makes the mosquitoes fluorescent just so that scientists can track them in the lab and in the wild and differentiate them normal mosquitoes. The second added gene is a gene that is passed to all the offspring of the GM mosquitoes and causes them to die before they reach adulthood.
The strategy is simple. Lots of male GM mosquitoes are released into an area. (It is only the female mosquitoes that bite and transmit disease.) The GM males compete with the natural males to mate with the natural females. The offspring of the GM males never make it to adulthood and the mosquito population plummets. Below some mosquito density, diseases can no longer be propagated from person to person because there are too few mosquitoes to guarantee that a sick person gets bitten and the disease is passed to the next person. These mosquitoes have been released in five trials in South America. Each time the local mosquito population was dropped by more than 90%. Since the GM mosquitoes and their progeny all die, the environment is not changed in any other way.
The only problem with this promising plan is public resistance. Residents in the Keys, like most Americans, have been conditioned for generations to be terrified of scientific words like “genetic” or “radiation”, and to believe that biotech is a synonym for “sinister poison” and corporation means “Beelzebub”. They are concerned that the GM mosquitoes will make their kids fluorescent or make them sterile or herald the zombie apocalypse.
So Oxitec is working on reassuring the good people of Florida by teaching them some basic high-school biology. They hope that they can make progress faster than Zika does. Time will tell.
The Hufnagel Heart Valve developed in the 1950s Credit: National Museum of Health and Medicine / Wikipedia
The aortic valve is the valve that allows blood out of the heart into the aorta, but not back. As people get older it’s not uncommon for the aortic valve to accumulate calcium deposits, stiffen, and not open as widely. This condition is called aortic stenosis. As the aortic valve narrows, it impairs the blood flow through it. Patients can develop heart failure, lightheadedness, chest pain, and fainting. There are no effective medications for aortic stenosis. Until several years ago the only treatment was valve replacement through open-heart surgery.
The first aortic valve replacement was performed in 1952. The initial mechanical aortic valves were plagued by blood clot formation, requiring patients to take high doses of anticoagulants (blood thinners) forever. Since then many incremental improvements have been made to prosthetic heart valves, but there was only one way to insert them – open-heart surgery. Surgery is quite effective, but it’s risky and has a prolonged recovery. Frail patients who have other medical problems frequently cannot tolerate the surgery. Up until a few years ago patients who could not undergo surgery would eventually die of worsening aortic stenosis.
Several years ago a new procedure for aortic valve replacement was developed. A catheter is placed in a large artery in the leg and threaded to the heart. The prosthetic aortic valve, folded via a miracle of origami engineering so that it can fit inside the catheter, is pushed through the catheter until it reaches the heart. A balloon is inflated to expand the valve into place. This procedure is called transcatheter aortic valve replacement (TAVR).
Since then, several studies have shown that for patients who cannot undergo open-heart surgery or are at extremely high risk from open-heart surgery, TAVR is an effective alternative. Initially TAVR was plagued by complications, but as cardiologists became more familiar with the procedure, and as the prosthetic valve itself incrementally improved (it’s already on its third version) the complication rate has fallen.
A study in 2013 found that about 67,500 aortic valve replacements were done through open-heart surgery every year, and that about 290,000 elderly patients with severe aortic stenosis were candidates for TAVR, with another 27,000 new patients becoming eligible for TAVR every year as their aortic valves worsen or as their health worsens, making surgery too dangerous.
In a rational marketplace, this would be cause for celebration. Hundreds of thousands of patients with a serious disease stand to benefit from a procedure that didn’t exist a decade ago. Their quality of life and possibly their longevity will be enhanced. The developers of the TAVR technology will make a lot of money. Everyone wins.
But our system is far from rational, because we all pay for each other’s stuff. Medicare is projected to become insolvent in the mid-2020s. The last thing the Medicare budget needs is a brand new very expensive procedure that hundreds of thousands of people can get. So Medicare established criteria to regulate who can undergo TAVR. For example, patients have to be examined by two cardiothoracic surgeons and have both of them decide that the patient is not a candidate for open-heart repair before Medicare will cover TAVR. It’s hard to justify these restrictions in terms of patient safety. These can only be motivated by thinly disguised rationing of a new and expensive procedure.
This month a new study in the New England Journal of Medicine (NEJM) compared TAVR to open-heart surgery in patients whose risk for surgery is not as high as in the initial studies. The study showed again that TAVR had equally good outcomes with much faster recovery.
For readers who follow technological change, this pattern is familiar. Open-heart surgery is a mature technology. Its radical breakthroughs and large incremental improvements happened decades ago. Surgical aortic valve replacement is very unlikely to undergo further drastic improvements. TAVR, on the other hand, is new, and is still in the early phase of exponential improvement. Think of word processors in the 90s, digital photography a decade ago, self-driving cars 10 years from now.
As the valve itself and the insertion technique improves, and as cardiologists build more experience, it’s reasonable to predict that TAVR will prove itself effective with patients at lower and lower risk for open-heart surgery. That is, patients who would be reasonable candidates for surgery may in a few years opt for TAVR.
Again, in a rational system this would be heralded as another example of Schumpeterian creative destruction. Surgically implanted valves could eventually go the way of the Polaroid Camera, the typewriter, the dial telephone. Cardiothoracic surgeons would find more productive things to do than replace aortic valves. Most importantly, patients would be much better off.
But instead, patients must now jump through bureaucratic hoops that were inappropriate when they were first implemented and now proven to be clinically unsound. Medicare will of course revise its restrictions, but this will take months, while sick patients wait.
We’re using a 1964 payment system to adjudicate coverage of twenty-first century procedures. Worse, we’re centralizing decision-making when all around us we see examples that leaving decisions to as many different people as possible yields the best outcomes. I would think that the best people to sort out how a patient’s aortic valve should be replaced are the patient’s cardiologist and the patient herself. And in a rational system, the price for TAVR would quickly fall (as it has for smart phones, and cars, and almost everything else you can think of) and she would put down her MasterCard to pay for it.
But instead, Medicare will slightly relax their byzantine rules, and many patients will unnecessarily undergo surgery rather than TAVR. And because of insurance coverage, prices will stay unaffordable indefinitely. And Medicare will still go bankrupt. Meanwhile, because the current system is both so unaffordable and so inadequate, and because some of us have boundless optimism about centralized decision-making, we are considering scrapping the current system and giving everyone Medicare.
Erythema migrans, the characteristic “bull’s-eye” rash of Lyme disease. Photo credit: CDC / James Gathany
Lyme disease is a bacterial illness transmitted by tick bites. It is treated with antibiotics, and most guidelines suggest a two to four week course of treatment. Most patients’ symptoms resolve at that point, but 10 to 20% of patients continue to have fatigue, joint and muscle pain, sleep problems, and difficulty concentrating. These patients can be quite debilitated and no specific effective treatment has been found for them.
A patient advocacy group has recommended treatment with antibiotics for months or even indefinitely for what they have called chronic Lyme disease. There has been scant data that such prolonged treatment is effective, and antibiotics can cause side effects and lead to antibiotic resistance. In fact four previous small trials have suggested that prolonged antibiotics do not improve outcomes. Many infectious disease experts doubt the existence of chronic Lyme disease and suggest that these patients may be suffering from a diverse group of other diseases, including chronic fatigue syndrome, fibromyalgia, and sleep disorders. (I wrote in 2007 about the chronic Lyme disease controversy.)
This week a study in the New England Journal of Medicine tried to answer definitively whether a prolonged course of antibiotics was helpful in patients with prolonged symptoms attributed to Lyme disease.
The study, which took place in the Netherlands, enrolled 281 patients with persistent symptoms attributed to Lyme disease. First, all the patients received two weeks of an antibiotic considered effective for Lyme disease. Then, the patients were randomized to three groups. Patients in the first group received 12 weeks of an antibiotic. Patients in the second group received 12 weeks of a different antibiotic. And patients in the third group received placebo for 12 weeks. Their symptoms were measured regularly for a year.
All three groups on average did equally well. Their symptoms improved steadily throughout the study. Unfortunately at the end of the study all three groups on average had a significantly worse quality of life than the general population. This brief video summarizes the findings.
What are we to learn? Well, first of all, prolonged antibiotics don’t help in patients with Lyme disease and persistent symptoms. But an interesting feature of the study helps draw a broader conclusion. The study enrolled patients that many infectious disease experts would not have diagnosed with Lyme disease. The symptoms required to enroll in the study can be caused my many diseases. The only link made in the study to Lyme disease is blood tests showing the presence of antibodies to the bacteria that causes Lyme. But these blood tests remain positive for decades after the disease has resolved. Many infectious disease experts would also require a history of a characteristic rash or the culturing of the culprit bacteria.
By avoiding these criteria the study enrolled many patients who might not have Lyme disease but who are frequently treated by self-styled Lyme disease advocates with prolonged antibiotics. Without making any judgment about the patients’ diagnosis, the study showed that this approach is futile.
I’ve had a few patients who’ve come to me with a diagnosis of chronic Lyme disease, frustrated that months of intravenous antibiotics (usually at enormous out-of-pocket expense) had failed to help them feel better. It’s difficult to say “I’m not sure what you have, and I’m not positive what will help.” But that’s what I’ve said, because that’s the truth. But I’m positive that they should stop the antibiotics.
Over 100 million doctor visits in the US each year result in a prescription for antibiotics. Over a third of those visits are for respiratory infections. A large fraction of the antibiotics prescribed yield absolutely no benefit to the patient. The issue is much more severe than just unnecessary spending on ineffective medication. As I’ve written before, antibiotic overuse is a major cause of emerging antibiotic resistance and of dangerous infections like Clostridium difficile. Antibiotics also can cause unpleasant side effects and (albeit rarely) life-threatening side effects.
ACUTE BRONCHITIS Symptoms: Cough that lasts up to 6 weeks with mild fever and aches. Causes: Most cases are caused by viruses. Role for antibiotics: None, unless pneumonia is present.
A generation ago we thought that colored phlegm was a sign of a bacterial infection. Now we know that the yellow or green phlegm is due to airway inflammation that can be caused by viruses or bacteria. Studies have shown that antibiotics for bronchitis don’t decrease the duration of cough and increase the rates of adverse events. If a doctor’s examination rules out pneumonia, antibiotics should be avoided.
PHARYNGITIS (THROAT INFECTION) Symptoms: Sore throat, pain swallowing, sometimes with fever. Causes: Usually caused by viruses. Some bacteria can also cause sore throats, most importantly Streptococcus. Role for antibiotics: Should only be prescribed if a Strep test is positive (with rare but important exceptions in adolescents and young adults).
The presence of cough, nasal congestion, pink eye, hoarseness, diarrhea, or cold sores make a viral cause much more likely. Even in cases in which the physical examination is consistent with Strep, many patient have a viral infection. So Strep should always be confirmed by culture or rapid testing before antibiotics are prescribed.
SINUSITIS (SINUS INFECTION) Symptoms: Nasal congestion with thick drainage, upper tooth pain, facial pain or pressure, fever, fatigue, ear pressure or fullness. Symptoms can last from a few days to a month. Causes: Most cases are caused by viruses, allergies, or irritants. Fewer than 2% of cases are bacterial. Role for antibiotics: Antibiotics should be prescribed if symptoms last more than 10 days, or severe or worsening symptoms last for 3 days.
Even in bacterial sinus infections, drainage of the sinuses frequently results in resolution of the illness. So decongestants like pseudoephedrine (Sudafed) or ipratropium (Atrovent) nasal spray are essential and usually curative. Antibiotics are a second line treatment if the decongestants alone don’t work.
COMMON COLD Symptoms: Sneezing, runny nose, sore throat, cough, low grade fever, headache, and malaise lasting up to 14 days. Causes: All colds are caused by viruses. Role for antibiotics: None.
Antibiotics don’t help colds. Zinc supplements have been shown to modestly reduce the duration of cold symptoms if taken less than 24 hours after symptom onset, but it can cause nausea and a bad taste. There is no evidence that vitamins (like C) and herbal remedies (like Echinacea) have any effect.
* * *
On this issue, societal interest and the welfare of individual patients are aligned. No one is asking patients to forego helpful medications for the sake of preserving the benefit of antibiotics for the future. On the contrary, patients are exposing themselves to harm and harming society when they take antibiotics for illnesses for which they have no benefit. So why are so many inappropriate antibiotic prescriptions written, and why do so many patients take them?
First, lots of patients grew up in an era when antibiotics were routinely prescribed for bronchitis and for sinus infections. We just didn’t know better then. The patients improved after taking these antibiotics (as they would have had they taken carrot soup or Tylenol or nothing) and are understandably convinced that antibiotics are required in these cases. Doctors have to educate these patients despite their entrenched expectations. Many doctors find that writing a prescription is faster than taking the time to teach.
Second, antibiotics give patients the (false) impression that they are doing something to hasten their recovery. The alternative – treating symptoms and waiting – can be very difficult when one is miserable. Doctors who are fully aware that antibiotics will be ineffective sometimes relent and prescribe them because it buys us ten days during which the patient accepts he’s on the road to recovery.
So patients owe it to themselves to be educated about when antibiotics work and when they don’t. And doctors owe patients an explanation about why antibiotics won’t help and how long it will take to recover. And then patients have to do the hard part and wait. That’s why we call you patients.